You've landed a meeting with a pharma company. You've rehearsed your pitch, polished your demo, and prepared for tough technical questions. But here's the question most health tech founders don't ask early enough: who exactly will be evaluating your solution — and what does each of them actually care about?
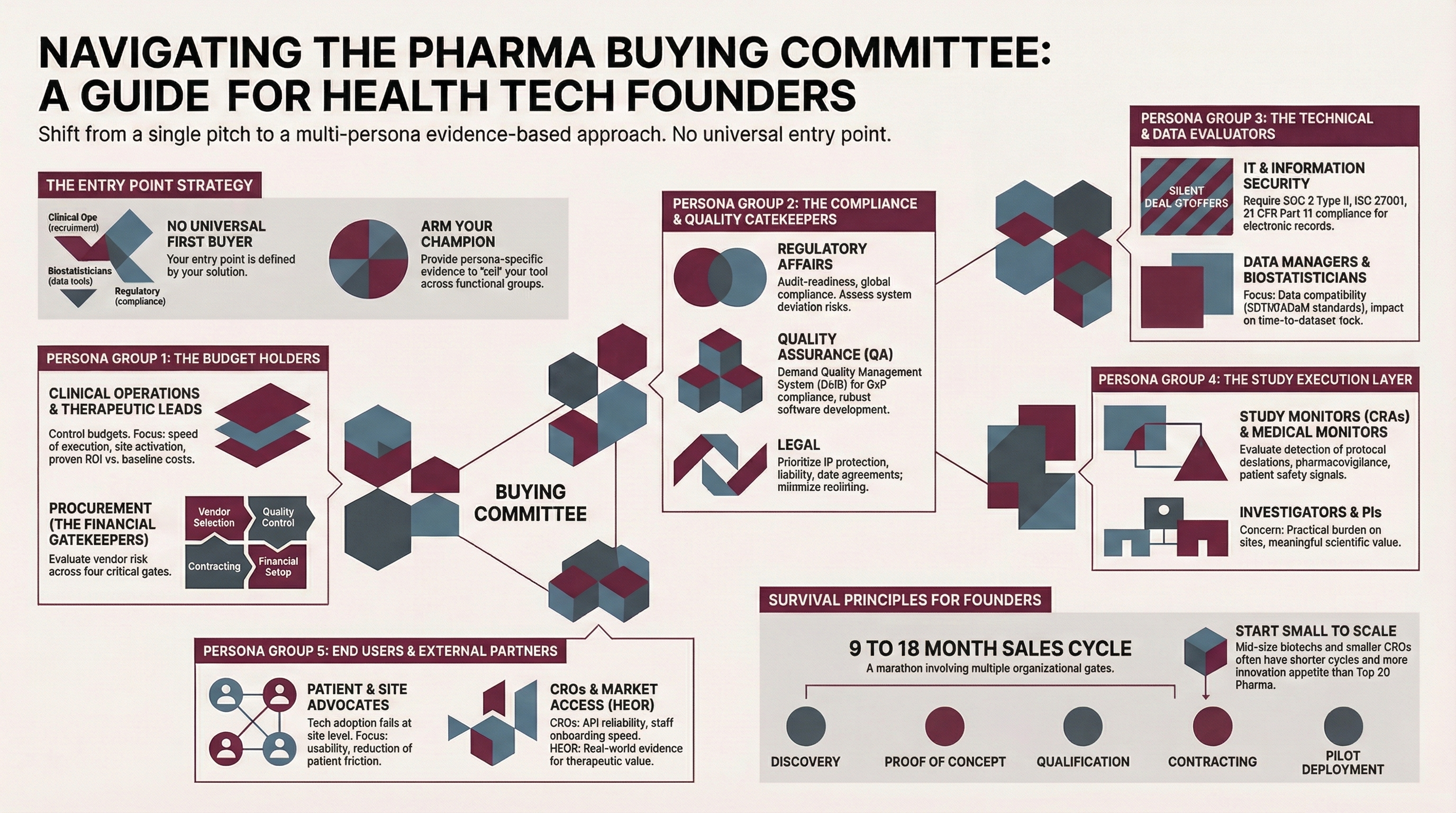
In pharma, there is no single buyer. There is a buying committee — a group of stakeholders from different functions, each evaluating your solution through a completely different lens. Research on B2B enterprise purchasing consistently shows that buying groups of six to ten decision-makers are common, and in large pharma organizations, that number can climb higher. Each stakeholder carries implicit veto power: if one function says no, the deal stalls.
The startups that succeed in this market are the ones that understand this reality early. They don't walk in with a single pitch; they walk in with a message that speaks to each seat at the table.
It Starts with Knowing Your Entry Point
Before we map the stakeholders, a critical reframe: there is no universal "first buyer" in pharma. Your entry point depends entirely on the problem your product solves.
If you're building a patient recruitment platform, your initial champion might sit in Clinical Operations. If you're building a tool that flags irregularities in clinical outcomes data, your first conversation is more likely with data monitors or biostatisticians. If you're offering a compliance automation tool, you might enter through Quality Assurance or Regulatory Affairs.
The entry point matters because it shapes the internal narrative. Your champion — whoever they are — will need to help sell your solution internally to all the other functions listed below. Your job is to arm them with the evidence each of those functions needs.
The Buying Committee: Who's at the Table
Every pharma and CRO organization is structured differently, but the core evaluating functions are remarkably consistent. Here's who you're likely to encounter — organized by the role they play in the decision.
The Budget Holders
Clinical Operations / Therapeutic Leads control the trial budgets and timelines. They care about speed of execution, site activation, enrollment performance, and whether adding your tool will deliver measurable value or simply add cost to an already tight budget. Don't assume they're your champion — especially if your product touches a workflow they feel is already working. They need to see proven ROI before they'll redirect budget to something new. Come prepared with quantifiable impact data: implementation time versus baseline, training completion rates, and concrete improvements in the metrics they already track.
Procurement evaluates vendor risk holistically — your financial health, operational track record, total cost of ownership, and whether engaging with you introduces dependencies the organization can't easily unwind. Ivanna Rosendal, VP and Global Head of Digitalization at Ascendis Pharma, has described the procurement journey candidly: four gates — vendor selection, quality control, contracting, and financial setup — each requiring documentation, each taking time, and together capable of outlasting a startup's financial runway. It's also worth noting that procurement is evolving at some organizations: R&D procurement teams increasingly include people with scientific backgrounds who evaluate "sourcing for innovation" rather than just cost containment. Where you encounter this kind of procurement partner, the conversation shifts from pure risk mitigation to strategic value — but don't assume this is the norm.
The Compliance and Quality Gatekeepers
Regulatory Affairs assesses whether your product supports or threatens audit-readiness and global regulatory compliance. They think in terms of ICH GCP guidelines, CDISC/ICH alignment, and submission readiness. They'll look at how many deviations your system introduces versus prevents.
Quality Assurance (QA) is a distinct function from Regulatory, though founders often conflate them. QA focuses on GxP compliance, your SOP adherence, your CAPA process, and audit findings. They want to see a Quality Management System that holds up under inspection. If your system generates or handles regulated data, QA will evaluate your validation documentation, change control processes, and how your software development lifecycle supports — or undermines — the sponsor's compliance obligations.
Legal evaluates liability, intellectual property, and contractual compliance. They care about redline-free contract execution, insurance coverage (E&O, cyber, general liability), and data processing agreements that will pass their review without months of negotiation.
The Technical and Data Evaluators
IT / Information Security are the gatekeepers for vendor qualification. Their review is formal, documented, and non-negotiable. At minimum, they'll look for SOC 2 Type II or ISO 27001 certification, along with your hosting architecture, encryption standards, access controls, penetration test results, and incident response protocols. For clinical trial technology specifically, they'll verify 21 CFR Part 11 compliance for electronic records and signatures. This is the function most likely to stop a deal quietly — they rarely attend the demo and may reject a vendor based entirely on documentation review. If your product uses AI or automation, expect an additional layer of scrutiny: some organizations now involve data privacy officers, AI governance committees, or responsible AI review boards in the evaluation, assessing ethical, legal, and algorithmic risks beyond traditional IT security.
Data Managers and Biostatisticians care about far more than integration. Yes, they need to know whether your system connects to their EDC, CTMS, and eTMF. But they're equally concerned with data compatibility — can your outputs map to SDTM and ADaM standards? How many queries does your system generate versus resolve? What does the time-to-dataset-lock look like? If your tool touches clinical data, these stakeholders will evaluate whether it improves or complicates the data pipeline from collection through submission.
The Study Execution Layer
Study Monitors / Clinical Research Associates (CRAs) are responsible for protocol adherence, data quality at the site level, and monitoring efficiency. They evaluate whether your technology will help them detect protocol deviations faster, resolve queries within SLA timelines, and maintain trial quality without adding monitoring burden. If your product touches data cleaning, risk-based monitoring, or site oversight, CRAs are a critical audience.
Medical Monitors focus on patient safety: adverse event and serious adverse event reporting timelines, MedDRA coding accuracy, and signal detection. If your product touches safety data in any way, medical monitors need to understand how it handles pharmacovigilance workflows.
Investigators and Principal Investigators care about scientific validity and the practical burden your tool places on their sites. They'll look at enrollment rates, protocol adherence, and whether your technology adds meaningful scientific value or just adds another system for their coordinators to learn.
The End Users and Partners
Patient and Site Advocates — whether a dedicated function or a perspective held by someone in Clinical Operations — evaluate usability from the ground up. Will site coordinators be able to use your tool without friction? Will patients find it accessible? Technology adoption fails most often at the site level, and as the industry moves toward hybrid trial models, the tools that win are the ones that reduce burden.
CRO and External Vendor Partners evaluate integration and workflow fit from the partner side — API reliability, data transfer accuracy, and how quickly their staff can onboard. If pharma's operational model involves a CRO running your tool, the CRO's assessment matters as much as the sponsor's.
HEOR and Market Access stakeholders, when involved, evaluate your solution's contribution to outcomes data — cost-per-patient improvement, quality-of-life measures, and real-world evidence that supports the broader value story of the therapeutic they're bringing to market.
This List Is Not Exhaustive
The stakeholders above reflect common patterns across pharma and CRO organizations, but every organization structures its buying committee differently. Some combine QA and Regulatory under a single leader. Some have dedicated innovation offices that serve as a front door for new vendors. Others involve finance teams, therapeutic area heads, or external advisory boards in the evaluation.
The point is not to memorize a fixed list. The point is to ask who will be evaluating your solution — and then prepare specific evidence for each of them.
When I work with clients, I use a Market Readiness Tracker to help them map the personas relevant to their specific product, identify each stakeholder's primary concerns and the KPIs they'll be measured against, and develop the talking points and assets needed to address them. It's one of the most valuable exercises a founder can do before entering the pharma sales process.
Preparing for the Committee
Map the buying committee before you walk in. Ask your initial contact who else will be involved in the evaluation. If they can't tell you, that's information in itself — the process may be earlier than you think, or your contact may not yet have internal sponsorship.
Prepare persona-specific materials. A single slide deck won't reach every function. Consider one-pagers tailored to specific audiences: an ROI summary for Procurement, a compliance and validation overview for QA and Regulatory, a data integration brief for IT and Data Management. Know your buying center and tailor your value proposition accordingly. Keep in mind the differences in organizational structures — startups move fast and act with agility, while large corporations often involve multiple hierarchical decision layers. Patience and persistence are key.
Respect the timeline. The typical sales journey — from first meeting through discovery, proof of concept, vendor qualification, contracting, and pilot deployment — spans nine to eighteen months. Building that timeline into your financial planning is not pessimism. It's survival.
Start where the barrier is lowest. Mid-size biotechs and smaller CROs often have shorter procurement cycles and more appetite for innovation. A successful pilot with a smaller organization builds the evidence base you'll need when a Top 20 pharma comes calling.
What Comes Next
Knowing who your buyers are is the first step. Understanding how they think — the shared psychology that drives pharma purchasing decisions across all of these functions — is the next. In the upcoming companion post, "Pharma Doesn't Buy Cool Tech: The Psychology of the Pharma Buyer," we'll explore why the most innovative product doesn't always win, and what pharma decision-makers are actually evaluating when they assess your solution.
